nailfold capillary
What is nailfold capillary?

aynaud’s phenomenon (RP) represents the most frequent clinical aspect of cardio/microvascular involvement and is a key
feature of several autoimmune rheumatic diseases. Moreover, RP is associated in a statistically significant manner with many
coronary diseases. In normal conditions or in primary RP (excluding during the cold-exposure test), the normal nailfold
capillaroscopic pattern shows a regular disposition of the capillary loops along with the nailbed. On the contrary, in subjects
suffering from secondary RP, one or more alterations of the capillaroscopic findings should alert the physician of the possibility
of a connective tissue disease not yet detected. Nailfold capillaroscopy (NV) represents the best method to analyse
microvascular abnormalities in autoimmune rheumatic diseases. Architectural disorganization, giant capillaries, haemorrhages,
loss of capillaries, angiogenesis and avascular areas characterize
>
95% of patients with overt scleroderma (SSc). The term
‘SSc pattern’ includes, all together, these sequential capillaroscopic changes typical to the microvascular involvement in SSc.
The capillaroscopic aspects observed in dermatomyositis and in the undifferentiated connective tissue disease are generally
reported as ‘SSc-like pattern’. Effectively, and early in the disease, the peripheral microangiopathy may be well recognized and
studied by nailfold capillaroscopy, or better with nailfold video capillaroscopy (NVC). The early differential diagnosis between
primary and secondary RP is the best advantage NVC may offer. In addition, interesting capillaroscopic changes have been
observed in systemic lupus erythematosus, anti-phospholipid syndrome and Sjogren’s syndrome. Further epidemiological and
clinical studies are needed to better standardize the NCV patterns. In future, the evaluation of nailfold capillaroscopy in
autoimmune rheumatic diseases might represent a tool for the prediction of microvascular heart involvement by considering the
systemic microvascular derangement at the capillary nailfold.
Introduction
The story of capillaroscopy ‘started’ from the observations of
an Italian physician, Giovanni Rasori (1766–1837), who described
the close relationship between conjunctival inflammation
and the presence of an ‘inextricable knot of capillary loops’ by a
magnifying glass [1].
During the beginning of the 20th century, Brown and O’Leary
[2] used the capillaroscopic analysis to show in detail the
abnormalities that characterize the involvement of microvascu-
lature during Raynaud’s phenomenon (RP) in systemic sclerosis
(Ssc). In 1973, Maricq

et al
. [3] published the first article in
Arthritis and Rheumatism
, describing the specific capillaroscopic
patterns in Ssc as well as the modification of the capillary
blood flow during cold exposure, both in primary and secondary
RP [3]. Nailfold videocapillaroscopy (NVC) represents the
best method to analyse micro/cardiovascular abnormalities in
rheumatic diseases. In normal conditions, the microvascular
pattern is characterized by a regular array of microvessels with
large intra/interindividual variability. However, absolute absence
of capillary loss and giant capillaries is expected in normal
pattern.
Recently, three defined major NVC patterns have been
considered useful in assessing the appearance and progression of
the sclerodermic microangiopathy (‘early’, ‘active’ and ‘late’
patterns) [4].
The ‘scleroderma pattern’
The microvascular damage in SSc is mainly characterized by
increasing structural alterations of the capillaries with progressive
decrease in their density [5, 6]. Blood flow is also altered, with an
average slowing of flow and increased periods of stasis.
Early in the disease, the peripheral microangiopathy may be
well recognized and studied by nailfold capillaroscopy or better
with the videocapillaroscopy, a non-invasive and safe technique,
which is well reported to have both diagnostic and prognostic
values in the presence of RP [6–11].
Previous studies have partially graded the morphological
aspects of the vascular damage in patients with SSc, as assessed
by nailfold capillaroscopy, and two major patterns within the term
‘scleroderma pattern’ (SSc pattern) have been recognized from
the beginning: namely the ‘active’ and the ‘slow’ patterns [7].
Further morphological studies have been published more
recently [12, 13].
In a recent study, microvascular alterations as detected by NVC
in patients with SSc have been re-classified in three different
patterns [4].
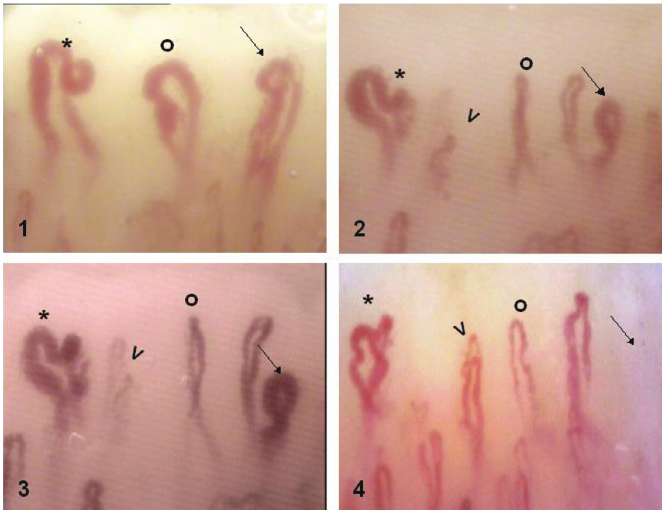
The patterns identified within the ‘SSc pattern’ include:
(i) ‘Early’ NVC pattern: few enlarged/giant capillaries, few
capillary haemorrhages, relatively well-preserved capillary
distribution, no evident loss of capillaries (Fig. 1); (ii) ‘Active’
NVC pattern: frequent giant capillaries, frequent capillary
Research Laboratory and Division of Rheumatology, Department of Internal Medicine, University of Genova, Viale Benedetto XV, 6, 16132 Genova, Italy.
Correspondence to: Maurizio Cutolo, Research Laboratory and Division of Rheumatology, Department of Internal Medicine, University of Genova,
Viale Benedetto XV, 6, 16132 Genova, Italy. E-mail: mcutolo@unige.it
Rheumatology 2006;45:iv43–iv46
doi:10.1093/rheumatology/kel310
iv43
ß
The Author 2006. Published by Oxford University Press on behalf of the British Society for Rheumatology. All rights reserved. For Permissions, pleas
e email: journals.permissions@oxfordjournals.org
haemorrhages, moderate loss of capillaries, mild disorganization
of the capillary architecture, absent or mild ramified capillaries
(
Fig. 2A); and (iii) ‘Late’ NVC pattern: irregular enlargement of
the capillaries, few or absent giant capillaries and haemorrhages,
severe loss of capillaries with extensive avascular areas, disorga-
nization of the normal capillary array, ramified/bushy capillaries
(Fig. 1).
This study confirmed previous observations, indicating
enlarged and giant capillaries together with haemorrhages as the
earliest NVC finding in SSc. In the late stage of the disease, these
abnormalities become rare.
Early stage is also characterized by microvessels with normal
diameter coexisting with few enlarged capillaries that must be
carefully investigated on all the fingers by considering the limited
number of these nailfold changes during early phases of the
disease [14–16].
Conversely, these changes are strongly increased in SSc patients
with an ‘active’ pattern. Loss of capillaries, together with vascular
architectural disorganization and ramified capillaries, were found
to be rare in the early stages of SSc, whereas they seem to increase
with the progression of the fibrotic phase of the disease (‘active’
and ‘late’ patterns).
A significant and gradual increase of these latter vascular
abnormalities is observed during the SSc progression, and the
three NVC patterns have been found to correlate with both RP
and SSc durations, reflecting at least the possible evolution of the
disease process [4].
While in healthy control subjects and in patients with primary
RP the morphological features of the nailfold microvascular bed
may remain unchanged for a long time, patients with RP
associated with SSc-spectrum disorders may, on the contrary,
show a higher degree of morphological variability, even after
a few days.
The NVC patterns have been correlated with different clinical
aspects and manifestations of SSc, as well as to the effects of
treatment contributing to the overall study of the disease [17–21].
Capillaroscopic patterns and rheumatic diseases
The presence of megacapillaries and a decreased capillary density
are the hallmarks of the SSc capillary pattern, which can be
detected by nailfold capillaromicroscopy.
However, in a recent large study, 186 patients with RP, 65 with
undifferentiated connective tissue disease (UCTD), 47 with
systemic lupus erythematosus (SLE), 26 with dermato/polymyo-
sitis, 14 with rheumatoid arthritis, 7 with primary Sjogren’s
syndrome (SS) and 102 patients with SSc were investigated [22].
Of the 16 patients with diffuse cutaneous SSc and the 86 with
limited cutaneous SSc, 14 (87.5%) and 53 (61.6%), respectively,
showed the SSc capillary pattern.
Nine of the 65 (13.8%) cases with UCTD and 24 of the
186 (12.9%) cases with RP also exhibited the same pattern.
Four of the 47 (8.5%) patients with SLE and seven of
the 26 (26.9%) with dermato/polymyositis, and no patients
with rheumatoid arthritis or SS exhibited the SSc capillary
pattern.
The conclusion is that the ‘SSc pattern’ is often present in
SSc and dermato/polymyositis. Furthermore, patients with RP
and UCTD may also exhibit this pattern occasionally (Fig. 2B).
Therefore, capillaromicroscopy seems to be a useful tool for the
early selection of those patients who are potential candidates for
developing SSc spectrum disorders.
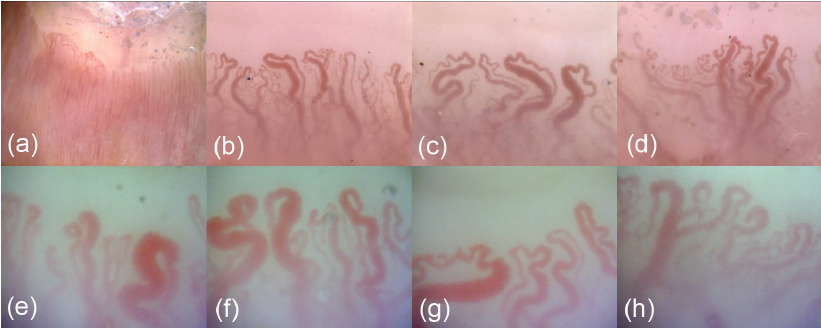
Dermatomyositis
A defined pattern has been reported in patients affected by
dermatomyositis (DM) [23]. This pattern, often associated with
aspects of the SSc pattern, includes the presence of two or more
of the following findings in at least two nail folds: enlargement of
capillary loops, loss of capillaries, disorganization of the normal
distribution of capillaries, ‘budding’ (‘bushy’) capillaries, twisted
enlarged capillaries and capillary haemorrhages (e
Nailfold capillary microscopy in connective tissue disease: a quantitative morphological analysis.
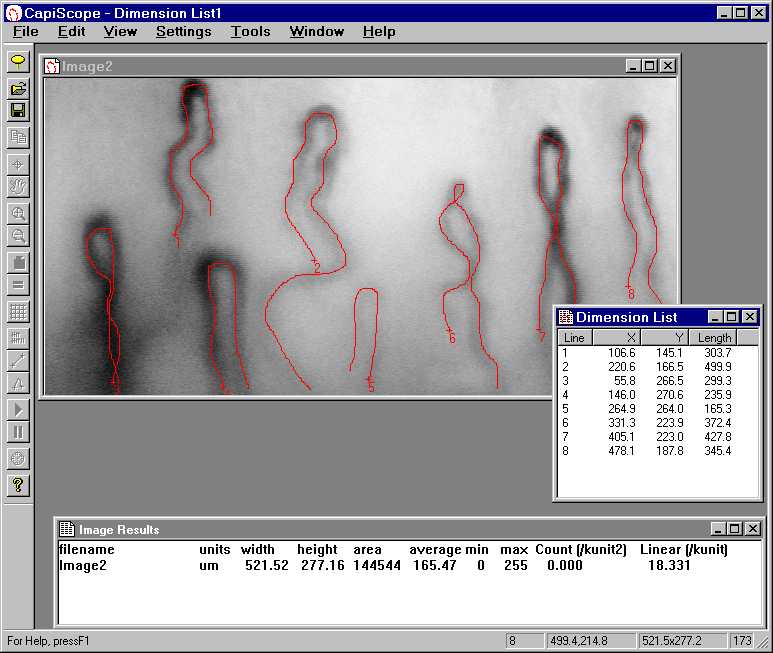
Photomicrographs were taken of front line nailfold capillary loops in 18 healthy women (controls) and 42 women with established connective tissue disease (14 rheumatoid arthritis, 19 systemic lupus erythematosus, nine scleroderma). Measurements were made of apex width, maximum limb and loop widths, capillary length, interpeak distance, and frequency per linear millimetre. A numerical index for assessing capillary dilatation was derived, based on the mean of the apex plus maximum limb widths. Results show considerable overlap in subject means. Statistical analysis showed no difference between rheumatoid arthritis and control groups. Patients with systemic lupus erythematosus had slightly larger loops at a lower frequency (not statistically significant); three patients with an abnormal capillary index also had high titres of ribonucleoprotein antibody. Six scleroderma patients had abnormal indices, two of whom had high titre ribonucleoprotein antibody. No relation between capillary morphology and clinical features was found.
nailfold capillary PDF
nailfold capillary
nailfold capillary Machine





Related Items