half and half nail syndrome
half and half nail syndrome-The yellow nail syndrome as originally described in 1964 by Samman and White1 presented a picture of diffuse yellow discoloration of the nail plate associated with lymphedema. In addition, there was a striking absence of cuticles and very slow nail-plate growth with both longitudinal and transverse overcurvature. Onycholysis proceeding to total shedding was also a prominent feature. Two years later, in 1966, Emerson2 added the finding of pleural effusion, completing the symptom triad as it is known today. This third manifestation often occurred together with sinusitis, bronchitis, and bronchiectasis.The half-and-half nail of Lindsay,3 first described in 1963 by Bean,4 detailed a nail-bed change in which the proximal half was white and the distal portion red to brown. This picture was noted most commonly in patients with chronic renal disease in whom serum nitrogen levels were usually elevated.
5 In addition to the nail-bed change, there may also be associated the presence of melanin in the acral part of the nail plate itself, thus involving a second component of the nail unit. The half-and-half nail may also be seen in patients without any demonstrable systemic abnormality.Half and half nails (also known as “Lindsay’s nails”) show the proximal portion of the nail white and the distal half red, pink, or brown, with a sharp line of demarcation between the two halves. Seventy percent of hemodialysis patients and 56% of renal transplant patients have at least one type of nail abnormality. Absence of lunula, splinter hemorrhage, and half and half nails were significantly more common in hemodialysis patients, while leukonychia was significantly more common in transplant patients.
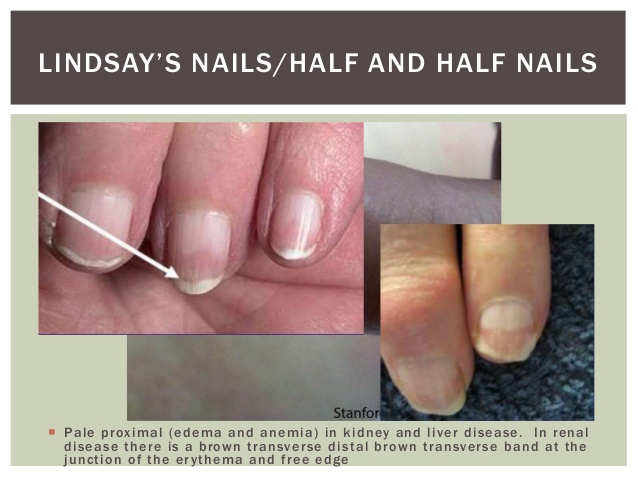
Half-and-half nail syndrome, also known as Lindsay nails, is one of the most characteristic, but not pathognomonic, onychopathies seen in chronic renal failure. Although the exact pathogenesis is unclear, it is speculated that acidosis and an increase in toxic uremic substances occurring subsequent to sudden renal decompensation may stimulate melanin formation by nail matrix melanocytes.While half-and-half nails affect an estimated 20% to 50% of chronic renal failure patients, a pattern has yet to be determined with regard to sex, age, and cause of the kidney disease. This entity is also seen in up to 84% of patients with azotemia and 8% to 13% of hemodialysis patients; there is some debate whether the frequency of these changes correlates with duration of dialysis. Other reported causes include Kawasaki’s disease, hepatic cirrhosis, zinc deficiency, and Crohn’s disease. Half-and-half nails have also been reported in patients without any systemic abnormality.Finger nails are affected more often than toe nails. The condition is characterized by a proximal pale pink or dull white “ground glass appearance” that is sharply demarcated from a red, pink, or brown distal portion. The transverse distal bands occupy 20% to 60% of the total nail length.There is no correlation between the distal band length and severity of renal failure. Furthermore, the half-and-half nail pattern appears to be persistent, as there is no tendency of the bands to move with nail growth. Nonetheless, this phenomenon may reverse itself after successful renal transplantation.
Half and half nail (brown arcs) is also known as Lindsay’s nail, in which proximal portion of the nail is white and the distal half (20-60%) is reddish brown. Although it was first described by Bean in 1963, Lindsay was the first to coin the term half and half nail in 1967. Baran and Gioanni were the first to correlate the half and half nail with renal disease and azotemia in 1968. It usually shows a sharp demarcation line between the two portions, which usually remains parallel to the distal free margin of the nail. There is no correlation between severity of azotemia and the distal band length. It is a rare but special clinical finding seen in chronic renal failure with a prevalence of 15-50%. It can also be seen in yellow nail syndrome, Crohn’s disease, Kawasaki’s disease, Behcet’s disease, cirrhosis, hyperthyroidism, zinc deficiency, citrullinemia, pellagra, HIV infection, and even in healthy persons.The exact pathophysiology of half and half nails is not well understood. The proposed theory is that an increase in capillary density along with capillary wall thickening is responsible for the development of the half and half nail rather than an increase in melanocytes.Treatment is only cosmetic as this is a benign condition that requires only counseling and reassurance. The transition band usually remains unchanged even after dialysis but disappears completely after successful renal transplantation. It usually takes 2-3 weeks for disappearance.
Related Items
